Fits, seizures and convulsions generally mean the same thing.
Seeing a child or young person having a fit can be frightening. Most fits do not cause serious harm. The commonest type of fit in children is a febrile convulsion. This is a fit associated with a high temperature. This sort of fit tends to occur in younger children. Fits sometimes occur without a fever (afebrile fit or seizure). If your child has had only one afebrile fit, it does not always mean they have epilepsy. Many children will never have another one.
First aid for a convulsive seizure:
A convulsive seizure is where the child is stiff or shaking. The information below can help you to focus when your child is having a seizure. It can help you to give first aid to keep them safe:
Do
• Stay calm
• Protect them from injury (remove harmful objects from nearby)
• Cushion or gently hold your child’s head to protect them from head injury
• Note the date and time the seizure started. If stiffness and jerking continues for 5 minutes or more you should call 999 for an ambulance
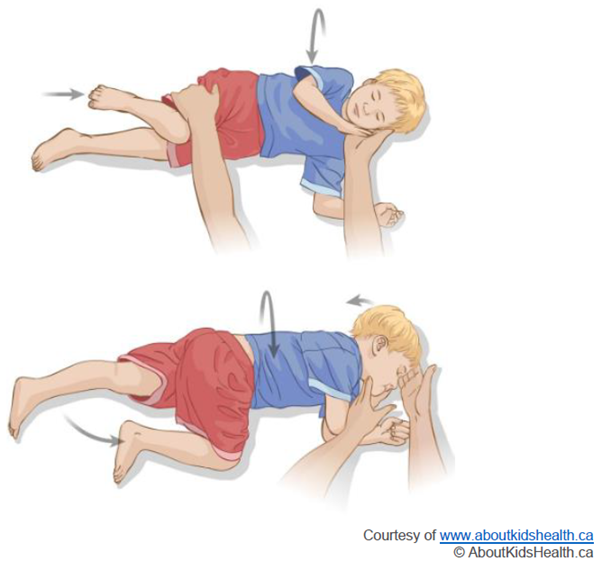
• Turn your child onto their side, into the recovery position (see below) as soon as you are able (as shown in Image 1). This can help with their breathing and help if they vomit or have other types of fluid in their mouth. Some noisy breathing and slight colour change is common
• If possible, try to video the seizure on a mobile phone as it can provide a lot of useful information to your child’s doctor or nurse. Video can help confirm the type of seizure which then helps decide which tests and treatment may be needed. Try to capture the whole child in the video, say out loud what you are seeing and show how they respond to you
• Stay with your child until they are fully recovered
• Your child may be confused, drowsy or fall asleep after a seizure. Reassure them if they are confused, let them rest or sleep if they are drowsy, make sure you keep an eye on them until they are fully recovered
Do not
• Restrain or restrict your child’s movements
• Move your child unless they are in danger
• Put anything in their mouth
• Give your child anything to eat or drink until they have fully recovered
Call 999 for an ambulance if:
• The stiffness or jerking continues for 5 minutes or more
• One seizure follows another before your child has fully recovered
• Your child is injured, or you are worried about their breathing
Moving a child into the recovery position: